Feminizing Top Surgery, also known as breast augmentation, is a common surgery to make the breasts larger and change their shape. Among trans women and trans feminine people, it can be an important step to address gender dysphoria and make the body match their sense of self. Four out of every five trans women report wanting or already having breast augmentation. The majority, over 80%, are satisfied with their results (de Block et al., 2020). Top surgery can also refer to chest reductions common among trans men and transmasculine people. We’ll use the term breast augmentation here to avoid confusion.
This procedure is very similar to the breast augmentations that cisgender women get. Any plastic surgeon who does augmentations for cis women should be able to do them for trans women and transfemminine people. There are a few relevant differences that may be more common for people who’ve gone through testosterone based puberty, compared to cisgender women. These can include:
- Asymmetrical growth, or one breast that’s noticeably larger than the other
- Nipples that are smaller and further apart, or look like they’re closer to the armpit than the center of each breast.
- Bigger chest muscles
- Wider sternum or space between breasts
An experienced surgeon will take these factors into consideration and discuss a plan for them.
Impact of HRT
You will usually need to be on feminizing HRT for at least a year (12 months) before getting a breast augmentation. Estrogen causes breast growth. Surgery will look more natural if you let hormones make your breasts grow as much as they can on their own. Many people recommend being on HRT for at least 2 years before seriously considering surgery.
Insurance companies also usually require you to be on HRT to cover surgery (Aetna, 2026). You may also need a letter from a mental health provider saying that you have gender dysphoria and are mentally prepared for surgery. Check with your insurance company to learn the specifics requirements for your plan. To learn more about HRT, check out last month’s blog post on the topic.
Types of Augmentation
There are three important factors to consider when deciding what kind of breast augmentation is right for you. The material that enhances the breasts will affect their size, shape, and firmness. Where the surgeon cuts into the body can determine scarring and options for revisions or additional enhancement in the future. The operative plane, or layer of tissue where the implant is placed, impacts healing time and how natural the long-term results look.
There are two procedures to enlarge the breasts- fat transfer (also known as lipofilling) and implants. Fat transfer takes fat from another part of the body, like the stomach, thighs, or butt, and moves it to the chest to make it fuller and larger. This newer technique can’t add as much size to the breasts as implants can.The body also reabsorbs roughly half of the fat that is transferred to the chest. This means your breasts may not stay as big as they were right after the procedure in the long term. Fat transfer may be a good option for people who want subtle, natural looking enhancement (Frankeny, 2024). It can also be combined with implants.
Implants are the go-to option for many trans women, because they can help add more size to the breasts than fat transfer alone. There are also two main types of implants- silicone and saline. Both have a soft, flexible silicone shell and are filled with silicone or saline (salt water). Silicone is thicker and may move more like natural breast tissue. However, silicone implants are restricted to people over 22 (Food and Drug Administration, 2019).
In the past, textured implants were also used. These are now linked to cause a type of lymph node cancer called breast implant-related anaplastic large cell lymphoma (BIR-ALCL). The brand Allergan recalled their Biocell implants in 2019 because of these concerns (Food and Drug Administration, 2024). If you currently have this type of implants, watch your chest for the following symptoms:
- Pain
- Lumps
- Swelling and fluid build up
- Skin discoloration on the breasts
- Unexpected changes in shape or texture of the breasts including asymmetry.
If you notice any of the above, talk to a plastic surgeon about having your implants removed or replaced (American Society of Plastic Surgeons, nd).
It’s also important to know that implants are only supposed to last for around 20 years.They will likely need to be replaced through another surgery in the future (Szymanski & Mikes, 2025). Ask your surgeon when you should plan to replace your specific implants.
There are three different places a surgeon can cut into the body to place breast implants. The Inframammary fold, or the crease where the breasts meet the abdomen, gives the surgeon the best view. However, scars may be visible if you have small breasts or when lying down. Periariolar incisions go around the nipple and areola. Your surgeon will use the difference in skin tones to hide the scar. This technique can cause loss of feeling in the nipples and may make it impossible to breastfeed. A transaxillary approach goes through the armpit and uses cameras to place the implant. It avoids scarring on the breasts and any potential nipple complications, but may be more expensive or make the surgery take longer. Scars may still be visible when you raise your arms.
Implants can be placed in one of two layers of tissue, or operative planes.
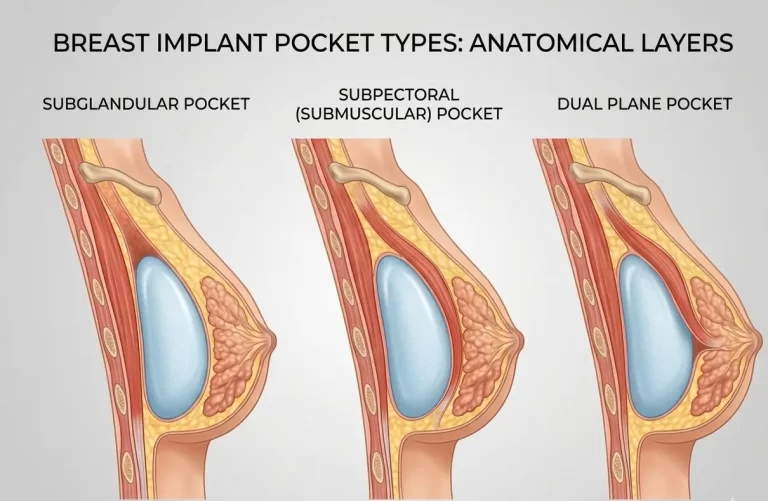
Subglandular implants go between breast tissue and the underlying muscle. They may heal quicker and more easily than implants in deeper layers. Because they are not as deep, you may be able to see wrinkles or ripples in the implant through the skin. Fat grafting is sometimes used to cover this. Subpectoral or submuscular implants go under the large muscle in the chest.This method takes longer to heal, and the implants may get higher on the chest over time (Strasser, 2006).
Risks & Potential Complications
Like any surgery, infection is one of the most common risks. It’s important to follow your surgeon’s aftercare instructions to help prevent infections.
There are two other common risks related to implants to know about if you’re interested in getting them. Around 1 in 10 breast implants will rupture within 15 years of getting them (Szymanski & Mikes, 2025). A rupture is a tear or hole in the silicone shell of the implant. This causes the saline or silicone inside of it to leak into your body. This is often caused by injuries, like car accidents.Your body can absorb saline safely, but silicone implants need to be removed or replaced quickly if they rupture. You should check for leaks in your implants three years after getting them. This is done using an MRI or ultrasound and isn’t typically covered by insurance.
Capsular Contracture is another risk of implants. It happens to about 1 out of ever 6 people who get a breast augmentation (Tehrani, 2018). Naturally occurring scar tissue around the implant gets hard and squeezes the implant. It can cause symptoms like:
- Pain in the breasts, especially when touched
- breasts that feel hard
- breasts that look higher on the chest than when you got the implants
- Mishapen nipples
If this happens, your breast augmentation may need to be redone.
Conclusion
To summarize, Feminizing top surgery (also known as breast augmentation) is a common surgery to make the breasts larger and change their shape. Breast augmentations are very safe surgeries with few potential complications. The majority of transfemmes who’ve gotten an augmentation are happy with the results. Insurance companies usually require you to be on HRT for at least a year before they will pay for augmentation. Some surgeons may not need this, but you may have to pay out of pocket. Three factors make each top surgery unique; type of implant, where the surgeon cuts, and what layer of tissue the implant is placed under. Each has pros and cons you will discuss with your surgeon.
Some common risks of breast augmentation include:
- Infection
- Implant ruptures or leaks
- Capsular contracture, or scar tissue that squeezes the implant
Next month’s CTH blog will help explain insurance coverage and preparing for gender affirming surgery.
References
Aetna. (n.d.). Clinical Policy Bulletins- Gender Affirming Surgery (0615). Retrieved April 17, 2026, from https://www.aetna.com/cpb/medical/data/600_699/0615.html
American Society of Plastic Surgeons. (n.d.). Allergan Biocell Device Withdrawal. American Society of Plastic Surgeons. Retrieved April 17, 2026, from https://www.plasticsurgery.org/patient-safety/breast-implant-safety/allergan-biocell-device-withdrawal
Bekeny, J. C., Zolper, E. G., Fan, K. L., & Del Corral, G. (2020). Breast augmentation for transfeminine patients: Methods, complications, and outcomes. Gland Surgery, 9(3), 788–796. https://doi.org/10.21037/gs.2020.03.18
Bekeny, J. C., Zolper, E. G., Manrique, O. J., Fan, K. L., & Del Corral, G. (2021). Breast augmentation in the transgender patient: Narrative review of current techniques and complications. Annals of Translational Medicine, 9(7), 611. https://doi.org/10.21037/atm-20-5087
de Blok, C. J. M., Staphorsius, A. S., Wiepjes, C. M., Smit, J. M., Nanayakkara, P. W. B., & den Heijer, M. (2020). Frequency, Determinants, and Satisfaction of Breast Augmentation in Trans Women Receiving Hormone Treatment. The Journal of Sexual Medicine, 17(2), 342–348. https://doi.org/10.1016/j.jsxm.2019.10.021
Food and Drug Administration. (2019, October 23). Types of Breast Implants. FDA. FDA. https://www.fda.gov/medical-devices/breast-implants/types-breast-implants
Food and Drug Administration. (2024, August 9). FDA takes action to protect patients from risk of certain textured breast implants; requests Allergan voluntarily recall certain breast implants and tissue expanders from market. FDA. FDA. https://www.fda.gov/news-events/press-announcements/fda-takes-action-protect-patients-risk-certain-textured-breast-implants-requests-allergan
Frankeny, A. (2024, November 18). Fat transfer for breast augmentation: The ins and outs of this implant alternative. American Society of Plastic Surgeons. https://www.plasticsurgery.org/news/articles/fat-transfer-for-breast-augmentation-the-ins-and-outs-of-this-implant-alternative
Strasser, E. J. (2006). Results of subglandular versus subpectoral augmentation over time: One surgeon’s observations. Aesthetic Surgery Journal, 26(1), 45–50. https://doi.org/10.1016/j.asj.2005.11.007
Szymanski, K. D., & Mikes, B. A. (2026). Breast Implant Rupture. In StatPearls. StatPearls Publishing. http://www.ncbi.nlm.nih.gov/books/NBK459308/
Tehrani, K. (n.d.). What is capsular contracture and how can it be treated? American Society of Plastic Surgeons. Retrieved April 17, 2026, from https://www.plasticsurgery.org/news/blog/what-is-capsular-contracture-and-how-can-it-be-treated