Gender Affirming Hormone Therapy, GAHT, is a medical treatment that uses hormones to help someone’s body align with their gender identity. It is one of the most effective and common treatments for Gender Dysphoria among trans and gender diverse (TGD) people. During puberty, hormones made by a person’s gonads (ovaries or testes) create changes in the body like a deeper voice, body hair, breast growth, and more. GAHT either replaces or suppresses these natural hormones. This includes feminizing hormones like estrogen for trans women and masculinizing hormones like testosterone for trans men. It may also include hormone blockers or medications to stop menstrual periods. These treatments are also sometimes called Hormone Replacement Therapy (HRT). This term includes other hormone treatments as well, like for menopausal cis women. While many people in the trans community use both terms, we’ll use GAHT here to prevent confusion.
Not all trans and gender diverse (TGD) people take GAHT. However, GAHT can improve mental health, self esteem, and quality of life for TGD adults and youth (Nguyen et al., 2018)! A trial of testosterone treatment among trans men showed reduced depression and suicidal thoughts in 3 months (Nolan et al., 2023). Further, 98% of TGD people on GAHT say they are more satisfied with their life than before taking it (James et al., 2024). If you are considering whether GAHT might be right for you, talk to a trusted healthcare provider.
Who prescribes GAHT?
The medications used in GAHT are only available with a prescription. GAHT is managed by a healthcare provider. This could be any of the following:
- family doctor, internist, or PCP
- endocrinologist
- gynecologist
- advanced practice provider like a Nurse Practitioner (NP) or Physicians Associate (PA)
It’s a common misconception that only endocrinologists can prescribe GAHT. Medical providers also don’t need special training or certification to provide GAHT. Certification is available through the World Professional Association for Transgender Health (WPATH), but it isn’t required to provide this care.
Some TGD people may get hormones through other means. For example, they may share prescriptions with friends and family, or buy them through international online pharmacies. These methods are sometimes called DIY (do-it-yourself) HRT/ GAHT. While many TGD people need DIY HRT if they can’t access an affirming provider, there are health risks to managing your own care. It’s also important to know that testosterone is a controlled substance. There may be legal risks to buying or selling it outside a pharmacy. Partnering with a healthcare provider is the safest, most effective option for GAHT.
What are the requirements to start GAHT?
GAHT is legal for adults (age 18+) in all U.S. States. To start treatment, adults have to give informed consent. This means they understand the risks, benefits, and alternatives to treatment and can make an informed decision about their healthcare. Check out this blog to learn more about informed consent. Your provider will also make sure you are healthy and don’t have any unmanaged medical conditions that would make GAHT unsafe. Before starting the medications, your doctor will do a physical exam and blood work. GAHT is customized based on labs and your personal goals. Taking GAHT also isn’t required for most gender-affirming surgeries.
It’s also important to know that GAHT is not a form of birth control, but may affect fertility. To avoid accidental pregnancy, sexually active people should use an effective form of birth control with GAHT. For transmasculine individuals, GAHT doesn’t affect what kinds of birth control you can take or how they work. Transfeminine people can use barrier methods, like condoms. More information about fertility and fertility preservation is available here.
Legal requirements for TGD youth are unfortunately more complex. Twenty-seven (27) states have passed a law that limits access to gender affirming care for TGD youth, including North and South Carolina. An estimated 50% of trans youth currently live in a state with limitations (Dawson & Kates, 2025). The Trans Youth Emergency Project monitors these laws and helps families find care in other states, when necessary.
Are there guidelines for GAHT?
Yes, several medical societies have published guidelines for the provision of this care.
Standards of Care (SOC) for the Health of Transgender and Gender Diverse People, Version 8 published by WPATH, is an important resource for health care professionals working with TGD patients. It provides detailed guidelines for the provision of gender affirming care, including GAHT. The Endocrine Society also provides guidelines for GAHT. Additionally, several medical societies have papers or statements supporting the use of GAHT.
Masculinizing HRT
For trans men and those who want a more masculine appearance, testosterone is used. The medication causes body changes like:
- increased body and facial hair growth
- voice deepening
- increase in muscle mass
- increased clitoral size (aka: bottom growth).
Testosterone can come as an injection or as a gel you rub on the skin. Changes start within a few months, but take several years to reach final results.
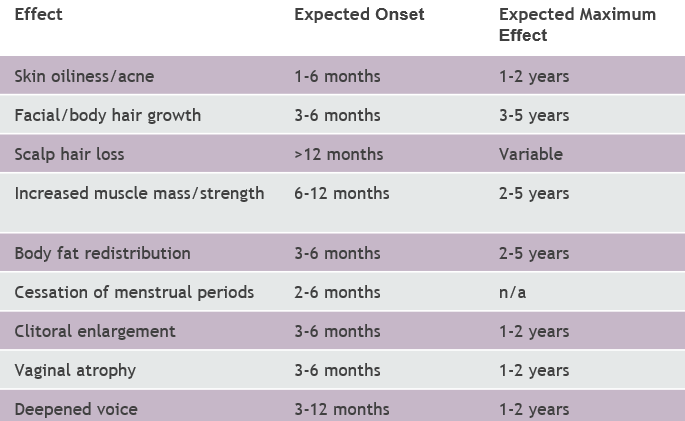
Side effects like acne and male-patterned hair loss may occur but are not dangerous. If these side effects bother you, talk to your doctor. They may be able to prescribe extra medications to help reduce side effects. While on testosterone your doctor will do blood work to ensure your dose of testosterone is right and that your blood count is in a safe range. When you start, labs will be every 3 months. These labs may only be needed once a year once your dose is stable. Labs reduce the risk of serious side effects like high red blood cell count which can cause blood clots, if not managed.
While testosterone does not provide birth control, it may reduce fertility. If someone gets pregnant while taking testosterone, there is a risk of birth defects. You should stop taking testosterone before trying to become pregnant.
Feminizing HRT
Estrogen is used for trans women and those looking for a more feminine appearance. Estrogen causes body changes like:
- breast growth
- softening of skin
- thinning body hair
- fat-redistribution in a more feminine pattern
Estrogen can come in a patch, pill, or injection. Changes begin within months, but take years to complete.
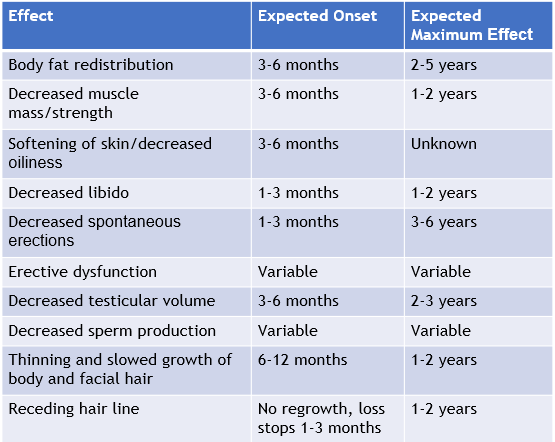
For estrogen to work, extra medications to lower testosterone are often needed. The most common testosterone lowering medication is a pill called spironolactone. Other medications may work better for some people. Some trans feminine people may also take progesterone. This medication may help with breast growth, sex drive/ libido, and mood swings, but more research is needed (Chang et al., 2025).
A common initial side effect of feminizing GAHT is a reduction in erections. This can cause sexual dysfunction. Your doctor can prescribe extra medications to help with this issue if it bothers you. Another possible rare side effect includes venous thromboembolism. This is a dangerous blood clot in the deep veins of the body. This is more common if you smoke cigarettes or use other kinds of nicotine, like vaping. The risk is lowest when estrogen levels are near the natural levels of cis women. To keep levels safe, medical providers check estrogen levels throughout treatment. When you start, this will be every 3 months. After your dose is stable, labs may only be needed once a year. Extra labs may also check testosterone levels, cholesterol, or liver/kidney function. The need for these depends on your health and your specific medications. Estrogen and testosterone lowering medications also limit your body’s ability to make sperm. This may reduce fertility during and after use.
Are the changes from GAHT permanent?
Yes, some changes from GAHT are permanent. The breast development caused by estrogen will not go away if you stop taking estrogen. Permanent changes from testosterone include:
- voice deepening
- facial and body hair growth
- scalp hair loss
- clitoral enlargement (bottom growth)
Other changes are reversible, like changes in body fat and muscle mass. The effects of GAHT on fertility are not fully understood. GAHT may reduce fertility and it may not return to “normal” if you stop taking GAHT.
Conclusion
To summarize, Gender Affirming Hormone Therapy (GAHT) is a treatment for Gender Dysphoria common among TDG people. It is prescribed and managed by a doctor or other healthcare provider. The provider will talk through the risks and benefits of GAHT and do blood tests before prescribing the medication to make sure it’s safe.
Trans men and masculine people take testosterone through injections or gel. It causes:
- Deepening of the voice
- Growth of facial and body hair
- Muscle growth and fat redistribution
- Loss of menstrual periods
- Clitoral enlargement (bottom growth)
Some of the side effects of testosterone include:
- Acne
- Hair loss on the head
- Too many red blood cells, which can cause dangerous blood clots
Trans women and feminine people take estrogen and testosterone blockers, usually spironolactone. Estrogen can come as pills, patches, injections, or gel. Other medications in feminizing GAHT are pills. These medications cause:
- Breast growth
- Fat redistribution
- Decreased muscle size/ strength
- Thinning body and facial hair
Some side effects of estrogen GAHT include:
- Erectile or sexual dysfunction
- Dangerous blood clots
Talking about side effects with your provider is important for your comfort and safety. Despite taking different medications, GAHT for trans women and trans men need labs every 3 months. After you’ve been on a steady dose, these follow-up appointments may only be needed once a year.
During the early stages of GAHT your body is going through a second puberty! It’s an exciting process many TGD people have waited years for. Starting GAHT may come with emotional changes as well as physical ones. While most people feel less depressed or anxious after starting, these symptoms may increase for some people. Trans women may be more likely to experience depression symptoms and mild mood swings after starting GAHT (Morssinkhof et al., 2024; Morssinkhof et al., 2025). Discuss any concerns with your medical provider or mental health provider. Our provider directory is a great tool for finding affirming doctors and therapists in the Charlotte area.
References
Coleman, E., Radix, A. E., Bouman, W. P., Brown, G. R., De Vries, A. L. C., Deutsch, M. B., Ettner, R., Fraser, L., Goodman, M., Green, J., Hancock, A. B., Johnson, T. W., Karasic, D. H., Knudson, G. A., Leibowitz, S. F., Meyer-Bahlburg, H. F. L., Monstrey, S. J., Motmans, J., Nahata, L., … Arcelus, J. (2022). Standards of Care for the Health of Transgender and Gender Diverse People, Version 8. International Journal of Transgender Health, 23(sup1), S1–S259. https://doi.org/10.1080/26895269.2022.2100644
Dawson, L., & Kates, J. (2025, November 24). Policy Tracker: Youth Access to Gender Affirming Care and State Policy Restrictions. KFF. https://www.kff.org/lgbtq/gender-affirming-care-policy-tracker/
Hembree, W. C., Cohen-Kettenis, P. T., Gooren, L., Hannema, S. E., Meyer, W. J., Murad, M. H., Rosenthal, S. M., Safer, J. D., Tangpricha, V., & T’Sjoen, G. G. (2017). Endocrine Treatment of Gender-Dysphoric/Gender-Incongruent Persons: An Endocrine Society* Clinical Practice Guideline. The Journal of Clinical Endocrinology & Metabolism, 102(11), 3869–3903. https://doi.org/10.1210/jc.2017-01658
James, S., Herman, J., Durso, L., & Hneg-Lehtinen, R. (2024). 2022 U.S. Trans Survey: Early Insights. National Center for Transgender Equality. https://ustranssurvey.org/
Morssinkhof, M. W. L., Schipper, M., Kreukels, B. P. C., van der Tuuk, K., den Heijer, M., van den Heuvel, O. A., Doyle, D. M., & Broekman, B. F. P. (2025). Changes in affect variability after starting gender-affirming hormone therapy. Psychoneuroendocrinology, 175, 107408. https://doi.org/10.1016/j.psyneuen.2025.107408
Morssinkhof, M. W. L., Wiepjes, C. M., van den Heuvel, O. A., Kreukels, B. P. C., van der Tuuk, K., T’Sjoen, G., den Heijer, M., & Broekman, B. F. P. (2024). Changes in depression symptom profile with gender-affirming hormone use in transgender persons. Journal of Affective Disorders, 348, 323–332. https://doi.org/10.1016/j.jad.2023.12.056
Nguyen, H. B., Chavez, A. M., Lipner, E., Hantsoo, L., Kornfield, S. L., Davies, R. D., & Epperson, C. N. (2018). Gender-Affirming Hormone Use in Transgender Individuals: Impact on Behavioral Health and Cognition. Current Psychiatry Reports, 20(12), 110. https://doi.org/10.1007/s11920-018-0973-0
Nolan, B. J., Zwickl, S., Locke, P., Zajac, J. D., & Cheung, A. S. (2023). Early Access to Testosterone Therapy in Transgender and Gender-Diverse Adults Seeking Masculinization: A Randomized Clinical Trial. JAMA Network Open, 6(9), e2331919. https://doi.org/10.1001/jamanetworkopen.2023.31919