Suicide Awareness Month
September is Suicide Awareness Month, which is intended to increase knowledge of and de-stgmatize this important mental health concern. While suicide has devastating impacts and an outsized effect on the LGBT community, there is hope. Resources and professional support are effective and available.
Suicide is defined as “intentionally ending one’s own life (Nock et al.,2008).” Suicidal thoughts and behaviors are terms that refer to a number of related concepts including considering suicide, making plans, and taking risks or harming one’s self with the intention of dying.
Scale of the Suicide Problem in the U.S.
Suicide is an urgent public health issue in the U.S. and causes an estimated 49,400 deaths each year (NIMH, 2025). Adolecents and young adults are at heightened risk for death by suicide– suicide is the second most common cause of death among all Americans ages 10-34 (CDC, 2023). Members of the LGBT community are also at higher risk for suicidal thoughts and behaviors than the general U.S. population. The Trevor Project estimates that more than 1.8 million LGBTQ+ young people (ages 13-24) in the U.S. seriously consider suicide each year (The Trevor Project, 2021). Among TGD people, an estimated 78% have considered suicide and 40% attempted suicide at some point in their lifetime compared to just 13.2% (considered) and 2.4% (attempted) of the US general population (Rastogi et al., 2025).
However, data on suicide deaths broadly and among LGBT people is likely underreported.ecause of the stigma associated with suicide, family members may obscure the nature of a person’s death (Fernandez & Jayawardhana, 2025). Additionally, the lack of standardized sexual orientation and gender identity data collection means that there is no reliable way to know if a person who died by suicide was LGBT after their passing. Despite the need for further research and improved data collection, we know a number of the factors that make LGBT people more likely to experience suicidal thoughts and behaviors.
LGBT Specific Risk Factors
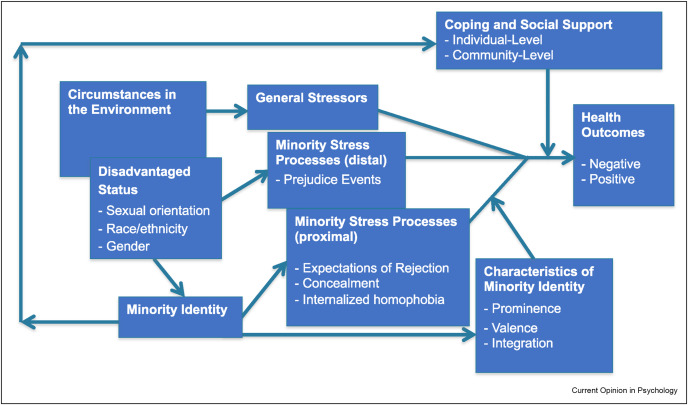
LGBT people face substantial discrimination, harassment, and victimization. The Gender Minority Stress Model posits that these external negative experiences combine with negative internal factors like expecting rejection from others, internalized transphobia, and gender dysphoria to create a higher likelihood of developing mental and physical health issues (Hendricks & Testa, 2012). Being transgender does not cause mental health issues or suicide; rather, the compounding, chronic stress and discrimination TGD people face is thought to be the cause of the elevated rates of negative mental health outcomes like depression, anxiety, and suicide.
Protective Factors & How to Help
Despite the significant impact suicide has on the LGBT community, we also know there are a number of protective factors, or things that help prevent it. Particularly for TGD youth, welcoming schools, affirming families, and accepting communities make a life saving difference; LGBT youth who described their home or school as affirming were significantly less likely to attempt suicide in the past year (The Trevor Project, 2024). Furthermore, connection to the LGBT community and Pride in one’s identity are connected to lower risk of suicidal thoughts and behaviors (Kanuika et al., 2019)
Everyone is capable of intervening in mental health crises and supporting their struggling loved ones. Recognizing some warning signs of suicide is the first step in preventing it (NAMI, 2022).
Warning signs can include:
- Saying things like: “I wish I wasn’t here”, “I wish I could go to sleep and never wake up”, or “Everyone would be better off without me”
- Mood swings
- Increased use of alcohol or drugs
- Impulsive or reckless behavior
- Isolating – not wanting to be around other people or do activities they used to enjoy
- Buying a weapon or collecting a large amount of medications
- Giving away their possessions, especially ones with sentimental value
- Making plans for pets, children, or other dependents
- “If anything ever happens to me, I’d want you to take care of my cat.”
- Getting legal/financial affairs in order
- Ex. a young, healthy person making a will; paying off debts
- Saying goodbye to family and friends
It’s a common misconception that talking about suicide will make someone more likely to attempt it; in fact, many people struggling with suicidal thoughts say it’s a relief for someone else to recognize the pain they’re in. To help the struggling person get the help they need, it’s important to ask directly if they’re thinking about suicide. If they say yes, calm, compassionate discussion comes next. Listen and validate their feelings without judgment. Sharing your own experiences can also help the person feel less isolated and offering resources can assist with getting them professional support. You could say things like:
“I had similar thoughts after my Mom passed away. I didn’t think there was any way out of the pain and grief until I started going to this support group. Would you like to go to a meeting with me next week?”
“I struggled with those kinds of feelings in the past. Talking to a therapist really helped. I still see them once a month, even though I’ve been doing a lot better lately. Can I call the office and see if another therapist there might be able to see you soon?”
Commit to checking in on them routinely, and offer resources. Asking for help can be scary and it may be helpful for you to be present to support them when trying to make an appointment with a therapist or calling a crisis line. Organizations like QPR and Mental Health First Aid also offer training on navigating mental health crises.
Always remember that there is hope; resources and help to address mental health challenges are life-changing and available. Together, we can create communities free of suicide.
Resources below (Charlotte area, NC state, National)
-Charlotte Area:
- Call: 704-444-2400
- The only dedicated psychiatric emergency department in the region
- Hours: 24/7
- Call: 704-566-3410 ext 1
- Hours: 24/7
-NC State:
- Call or Text: 877-235-4525
- Hours: 24/7
- Call: 211 or 1-888-892-1162
- NC 211 is an information and referral service provided by United Way of North Carolina and powered by local United Ways of North Carolina. Families and individuals can call to receive free and confidential information on health and human services within their community.
- Hours: 24/7
- NC Peer Support Warmline
- Call: 1-855-733-7762
- Offers a peer crisis hotline, and respite for folks seeking to avoid psychiatric hospitalization
- Hours: 24/7
-National:
- Call: 800-604-5841
- Hours: 24/7
- Crisis Text Line
- Text: HOME to 741741
- Website: https://www.crisistextline.org/
- Hours: 24/7
- LGBT National Help Center (see link for different chat and hotline options and hours)
- Website: http://glbtnationalhelpcenter.org/
- Hours: NOT 24/7 – visit website for details
- Call or Text: 988
- Hours: 24/7
- Call 844-762-8483
- Hours: 24/7
- The Trevor Project (ages 13-24)
- Call: 866-488-7386
- Text: Text the word START to 678-678
- Hours: 24/7
- Call: 877-565-8860
- Hours: 24/7
- Call: 888-407-4515
- 7pm to 9pm ET Monday through Thursday
- 7pm-10pm ET Friday through Sunday
References:
Centers for Disease Control and Prevention. (2023). WISQARS Leading Causes of Death Visualization Tool. Centers for Disease Control and Prevention. https://wisqars.cdc.gov/lcd/
Fernandez, J. M., & Jayawardhana, J. (2025). Are suicides underreported? The impact of coroners versus medical examiners on suicide reporting. Health Services Research, 60(2), e14381. https://doi.org/10.1111/1475-6773.14381
Frost, D. M., & Meyer, I. H. (2023). Minority stress theory: Application, critique, and continued relevance. Current Opinion in Psychology, 51, 101579. https://doi.org/10.1016/j.copsyc.2023.101579
Hendricks, M. L., & Testa, R. J. (2012). A conceptual framework for clinical work with transgender and gender nonconforming clients: An adaptation of the Minority Stress Model. Professional Psychology: Research and Practice, 43(5), 460–467. https://doi.org/10.1037/a0029597
Kaniuka, A., Pugh, K. C., Jordan, M., Brooks, B., Dodd, J., Mann, A. K., Williams, S. L., & Hirsch, J. K. (2019). Stigma and suicide risk among the LGBTQ population: Are anxiety and depression to blame and can connectedness to the LGBTQ community help? Journal of Gay & Lesbian Mental Health, 23(2), 205–220. https://doi.org/10.1080/19359705.2018.1560385
Kim, R., Wagner, E., Nestadt, P., Somayaji, N., Horwitz, J., & Crifasi, C. (2025). Gun Violence in the United States 2023: Examining the Gun Suicide Epidemic. Johns Hopkins Bloomberg School of Public Health.
National Alliance on Mental Illness. (2022). Risk of Suicide. National Alliance on Mental Illness (NAMI). https://www.nami.org/about-mental-illness/common-with-mental-illness/risk-of-suicide/
National Institute of Mental Health (NIMH). (2025). Suicide. https://www.nimh.nih.gov/health/statistics/suicide
Nock, M. K., Borges, G., Bromet, E. J., Cha, C. B., Kessler, R. C., & Lee, S. (2008). Suicide and Suicidal Behavior. Epidemiologic Reviews, 30(1), 133–154. https://doi.org/10.1093/epirev/mxn002
Rastogi, A., Menard, L., Miller, G., Cole, W., Laurison, D., Caballero, J., Murano-Kinney, S., & Heng-Lehtinen, R. (2025). Health & Wellbeing: Findings from the 2022 U.S. Trans Survey. Advocates for Trans Equality. https://ustranssurvey.org/download-reports/
The Trevor Project. (n.d.). 2024 U.S. National Survey on the Mental Health of LGBTQ+ Young People. 2024 National Survey on LGBTQ+ Youth Mental Health. Retrieved August 27, 2025, from https://www.thetrevorproject.org/
The Trevor Project. (2021, December 15). Facts About Suicide Among LGBTQ+ Young People. The Trevor Project. https://www.thetrevorproject.org/resources/article/facts-about-lgbtq-youth-suicide/